
Dysplastic Nevus Decoded: A Plain-Language Guide to Atypical Moles, Cancer Risk, Monitoring, and When Removal Is Needed
Learn what a dysplastic nevus (atypical mole) really means, its cancer risk, how often to monitor, and when removal is necessary—explained in simple language.
Why This Topic Matters
You go for a skin check. The dermatologist looks at one of your moles and says, “This looks like a dysplastic nevus.” You nod politely… but inside, you’re confused. Is it cancer? Is it going to become cancer? Should it be removed right now?
You’re not alone. Many patients hear the term dysplastic nevus and leave with either unnecessary fear (“I have pre-cancer!”) or false reassurance (“It’s just a mole, ignore it”). Both reactions can be harmful.
This article explains dysplastic nevi (also called atypical moles) in clear, everyday language. We’ll cover:
What a dysplastic nevus actually is
How it differs from a normal mole
Real cancer risk (not exaggerated, not minimized)
How often you should monitor these moles
When removal is needed—and when it isn’t
Pros and cons of monitoring vs removal
The goal is simple: help you understand what is happening on your skin so you can make calm, informed decisions.
What Is a Dysplastic Nevus (Atypical Mole)?
A dysplastic nevus is a mole that looks different from common moles. It is not cancer. But it is also not a completely typical mole.
Think of it like this:
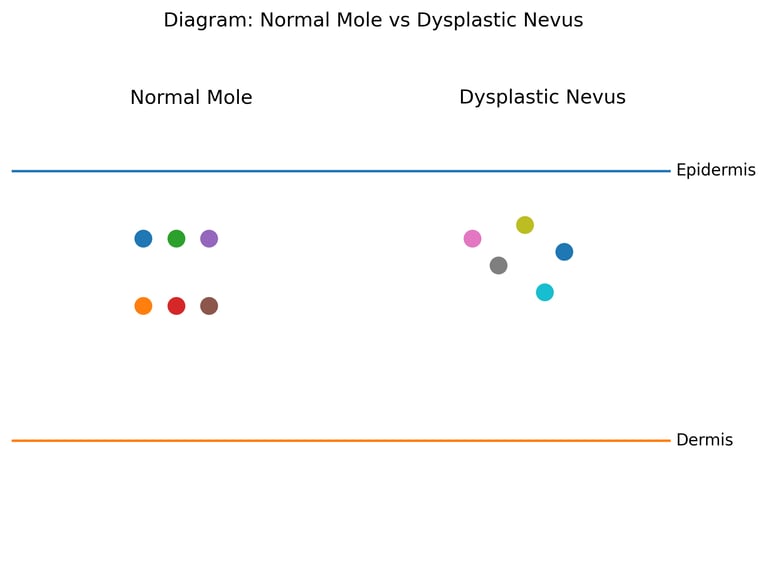
A normal mole is like a well-behaved student in class—neat, uniform, predictable.
A dysplastic nevus is the creative student—still following rules, but with unusual patterns and variations.
It may look:
Slightly larger than common moles
Uneven in color (light brown + dark brown + pink)
Irregular in shape
Fuzzy or poorly defined at the edges
This “atypical” appearance is what makes doctors pay closer attention.
Important Truth
A dysplastic nevus is not automatically pre-cancerous.
It simply means the mole has some unusual features that need monitoring.
First, Understand a Normal Mole (So You Know What’s “Different”)
Before we talk about what’s abnormal, we must understand what a normal mole is.
The Normal Skin Cell Story
Your skin has special pigment cells called melanocytes. Their job is to produce melanin—the pigment that gives your skin its color and protects against UV rays.
Normally:
Melanocytes are evenly spaced
They grow in an organized pattern
They stop multiplying when they should
When a mole forms, melanocytes cluster together. This is still normal behavior, just in a small grouped pattern.
So a normal mole:
Is symmetrical
Has one color
Has smooth borders
Remains stable over time
This organized pattern is like bricks laid neatly in a wall.
What Makes a Dysplastic Nevus “Atypical”?
Now imagine those same bricks placed unevenly:
Some darker, some lighter
Some slightly out of alignment
Edges not perfectly straight
That is essentially what happens in a dysplastic nevus.
The melanocytes are still controlled, but their pattern is less orderly. They may vary in:
Size
Shape
Color distribution
This uneven pattern is why doctors label them “atypical.”
Key Point
The cells are unusual—but not behaving like cancer cells.
They are more like a messy bookshelf than a burning house.
Are Dysplastic Nevi “Pre-Cancerous”?
This is the most misunderstood part.
The Balanced Truth
Most dysplastic nevi never turn into melanoma
But people who have many dysplastic nevi have a higher lifetime risk of melanoma overall
So the mole itself is not guaranteed to become cancer. Instead, it acts as a risk marker, like a warning sign that says:
“Pay closer attention to your skin.”
A Simple Analogy
Owning one dysplastic mole is like having one pothole on the road.
Having many dysplastic nevi is like driving on a road with multiple potholes—you’re more likely to hit a serious one eventually.
The risk depends on:
Number of atypical moles
Family history of melanoma
Sun exposure habits
Skin type (fair skin burns easier)
Genetics and Family Risk
Some people inherit a tendency to develop many atypical moles. This is sometimes called familial atypical mole syndrome.
Imagine your skin cells have a “growth brake system.”
In some families, this brake system is slightly weaker due to inherited gene changes. The cells still stop growing—but not as neatly as usual.
This does not mean cancer is guaranteed. It only means:
More frequent skin checks are wise
Sun protection becomes especially important
If multiple family members have:
Numerous atypical moles
Or melanoma history
Then professional monitoring becomes essential.
Who Is More Likely to Have Dysplastic Nevi?
You are more likely to have atypical moles if you:
Have fair skin that burns easily
Have many total moles (50+ on body)
Have a family history of melanoma
Had intense sunburns in childhood
Use tanning beds (strong evidence shows increased melanoma risk)
These are risk factors—not destiny.
How to Recognize a Dysplastic Nevus at Home
Doctors often use the ABCDE guide to identify suspicious moles.
ABCDE Reminder (Simplified)
A = Asymmetry (one half unlike the other)
B = Border irregularity
C = Color variation
D = Diameter larger than ~6 mm (pencil eraser)
E = Evolving (changing over time)
But here’s the nuance:
A dysplastic nevus can show some ABCDE features yet remain benign. That’s why professional evaluation matters.
How Often Should You Check?
This depends on personal risk level.
General Guidance
If you have:
1–2 atypical moles → yearly skin exam
Multiple atypical moles → every 6–12 months
Family history of melanoma → every 6 months (or as advised)
Dermatologists may also use:
Dermoscopy (magnified skin exam)
Total body photography (baseline mole mapping)
These tools help detect subtle changes early, without removing every mole unnecessarily.
How to Perform a Self Skin Check (Step-by-Step)
Monthly self-checks are powerful and evidence-based.
Stand in good lighting with a full-length mirror
Check face, neck, chest, and arms
Use a hand mirror for back and scalp
Look at palms, soles, nails, and between toes
Compare moles to previous photos if available
You are looking for:
New mole appearing after age 30
Rapid change in size or color
Itching, bleeding, or crusting
These signs should prompt a dermatology visit.
When Does a Dysplastic Nevus Need Removal?
Not every atypical mole must be removed. This is a common myth that leads to unnecessary procedures.
Removal is recommended when:
The mole changes over time
It looks suspicious under dermoscopy
It differs from your other moles (“ugly duckling” sign)
Biopsy shows moderate-to-severe cellular atypia
Patient anxiety is high after counseling (shared decision-making)
Important Insight
Stable dysplastic nevi can safely be monitored instead of removed.
What Happens Inside the Mole?
To understand “what is wrong,” we must first understand normal structure.
Normal Skin Structure
Your skin has layers:
Epidermis: top protective layer
Dermis: deeper support layer
Melanocytes sit at the junction of these layers, like border guards controlling pigment distribution.
They usually:
Stay evenly spaced
Grow in small, orderly nests
Stop multiplying at the right time
What Changes in a Dysplastic Nevus?
In an atypical mole:
Melanocytes vary slightly in size and shape
Nests of cells may be uneven
Cells may spread along the junction in a less organized pattern
But crucially:
They still respect the body’s control signals.
They are unusual—but not invading like cancer cells do.
Think of it as slightly disorganized construction, not uncontrolled demolition.
Treatment Options
1. Surgical Excision (Complete Removal)
How it works
The mole is cut out with a small margin of normal skin. This ensures complete removal and allows microscopic examination.
Effectiveness
Very high. Once completely removed, that mole cannot become melanoma.
Healing Time
Stitches removed in 1–2 weeks
Scar fades over months
Possible Side Effects
Scar formation (most common)
Infection (rare)
Pigment change around scar
Who Should Consider Excision?
Suspicious or changing mole
Strong family history of melanoma
Pathology showing severe atypia
Who Should Avoid Unnecessary Excision?
People with many stable atypical moles
Those prone to keloid scars
When mole appearance is unchanged for years
2. Shave Removal
How it works
The top portion of the mole is shaved off at skin level.
Limitations
May not remove deeper cells
Mole can regrow
Harder to evaluate margins fully
This method is often used when melanoma risk is low but cosmetic removal is desired.
Pros and Cons: Monitoring vs Immediate Removal
Monitoring (Observation)
Pros
Avoids unnecessary scars
Safe for stable atypical moles
Allows long-term pattern comparison
Cons
Requires regular check-ups
Can cause anxiety in some patients
Removal (Excision)
Pros
Eliminates that mole’s cancer potential
Provides definite diagnosis
Cons
Leaves scar
Not practical for patients with dozens of atypical moles
Small surgical risks
The best choice depends on individual risk and patient comfort level.
Lifestyle and Habit Changes That Actually Help
Evidence strongly supports these protective measures:
Sun Protection (Most Important)
UV exposure is a major trigger for melanoma development.
Practical steps:
Use broad-spectrum sunscreen SPF 30+ daily
Reapply every 2 hours outdoors
Wear hats and protective clothing
Avoid tanning beds (strong melanoma link)
Seek shade between 10 AM–4 PM
These habits reduce cumulative skin damage over time.
Diet and Supplements
No specific food can remove dysplastic nevi.
However, diets rich in fruits, vegetables, and antioxidants support general skin health. Evidence supports overall balanced nutrition—not miracle supplements.
Common Myths About Dysplastic Nevi
Myth 1: “It will definitely become cancer.”
Reality: Most never do.
Myth 2: “Every atypical mole must be removed.”
Reality: Stable ones can be safely monitored.
Myth 3: “If it was removed once, I’m no longer at risk.”
Reality: Risk depends on your overall skin pattern, not one mole.
Disease Associations to Be Aware Of
Having multiple dysplastic nevi may be associated with:
Increased melanoma risk
Familial atypical mole syndrome (rare but important)
This does not mean cancer is inevitable. It simply means vigilance matters.
Who Should Consider Extra Careful Monitoring?
You should be especially proactive if you:
Have more than 50 moles
Have several atypical moles
Have a family history of melanoma
Had repeated childhood sunburns
Notice frequent mole changes
These individuals benefit most from regular dermatology visits.
Real-World Implications for Everyday Life
For most people, dysplastic nevi mean:
More awareness, not panic
Regular monitoring, not aggressive surgery
Sun protection, not lifestyle restriction
You can live a completely normal life while simply being more observant of your skin.
Who Should Consider This Information Most Relevant?
This guide is especially useful for:
Patients told they have “atypical moles”
Individuals with many moles on their body
Families with melanoma history
People worried whether their mole is “pre-cancerous”
Understanding removes fear—and prevents neglect.
Conclusion
A dysplastic nevus is best understood as a “mole that deserves attention, not alarm.” It is not cancer. It is not guaranteed to become cancer. But it does signal that your skin may need closer monitoring than average.
The smartest approach is balanced:
Do not panic and remove every atypical mole
Do not ignore changes over time
Practice consistent sun protection
Perform monthly self-exams
Follow dermatologist-recommended check intervals
Removal is necessary only when a mole changes, looks suspicious, or shows significant cellular atypia under the microscope. Otherwise, careful observation is a safe and evidence-based strategy.
In simple terms:
A dysplastic nevus is a yellow traffic light—not red, not green.
It tells you to slow down, stay alert, and keep watching the road ahead.